If 2025 felt like a year where many ACOs coasted to shared savings, 2026 is already shaping into something else entirely. Spending is rising faster than expected, CMS is recalibrating the ground rules, and the old margin cushions are thinner than ever. CFOs can feel the slope changing underneath them.
The Medicare Shared Savings Program will still reward accountable care organizations, but the winners will look different. They will operate with tighter decision cycles, better forecasting, and a level of coordination that fee for service organizations rarely achieve. The rest will rely on hope, and hope is an expensive strategy.
Below are the shifts defining the year ahead, when the reality of risk and opportunity comes into sharper focus.
1. The Benchmark Era Of Easy Wins Is Ending
Many ACOs celebrated record shared savings in 2025, yet almost everyone knew the math was inflated. Actual Medicare spending grew 7.1%, while ACPT benchmarks rose 4.9%. Clearing that bar felt good at the time, but it set a trap.
CMS will tighten these benchmarks in 2026. That means CFOs need to understand what portion of their savings came from performance and what came from benchmark generosity. Organizations baselining their true position now will walk into future participation agreements with clarity. Those who delay may find themselves negotiating blind.
2. Compliance Is Beginning To Behave Like A Revenue Lever
Most health care providers talk about compliance as something that must be done to stay out of trouble. Yet some organizations have discovered a more strategic truth. The January 2026 Interoperability Rule forces API adoption, and while the penalties get attention, the hidden benefit often matters more.
Organizations that rebuilt prior authorization and data workflows during compliance preparation saw denials drop by 15 to 25% and recovered millions in preventable leakage. Compliance began to behave like a cost reduction mechanism. Seeing it that way changes everything.
3. Labor Pressures Are Quietly Rewriting Operating Models
Anyone responsible for staffing feels the tension. Physicians spend nearly 13 hours a week on prior authorizations, and a third say they may leave the field within five years. Labor already accounts for 56% ($890B) of hospital costs. When people are stretched this thin, the financial risk rises in ways spreadsheets do not fully reflect.
This is why more organizations are shifting non-clinical functions outward.
Revenue cycle work, IT operations, compliance monitoring, and analytics are moving to specialized partners who can operate at 40 to 60% of internal cost. The goal is not to reduce headcount. It is to preserve the workforce needed to deliver high quality care to Medicare enrollees while lowering costs in the Medicare program.
4. Documentation Is Becoming One Of The Purest Sources Of Hidden Revenue
Walk through any health system and you can see the same story unfold. Coders fixing old records. CDI teams chasing down missing details. Leaders trying to explain revenue patterns that do not match the case mix.
Clinical documentation creates a hidden drain on organizational resources. Physicians devote 34 to 55 percent of their workday to documentation in electronic health records, costing U.S. healthcare systems $90 to $140 billion annually in lost productivity. Time that could otherwise be directed toward patient care. In 2026, the organizations moving ahead are the ones treating documentation as a proactive asset rather than a compliance burden.
AI supported documentation captures more clinical complexity and cuts query volume, which often leads to CMI lifts of 5 to 15%.
That is real money, both in recovered revenue and reclaimed physician time. And it comes from work that clinicians are already doing.
5. Predictive Analytics Is Becoming The New Advantage
There is a moment when a CFO realizes that most value based care forecasting is backward looking. Only a minor percentage of providers trust their population health data accuracy. That uncertainty leaks shared savings.
Predictive analytics changes the dynamic. When organizations can identify rising risk patients, anticipate spending targets, and model intervention ROI, execution becomes steadier.
Black Road Health exemplifies this shift. By partnering with Humbi AI to access comprehensive Medicare and Medicaid data spanning 200+ million lives and combining it with advanced actuarial analytics, Black Road Health transformed their forecasting precision. They gained the ability to model multiple scenarios, predict spending trends, and make data-driven decisions with confidence.
As founder Sunil Cardozo said: "They access Medicare and Medicaid commercial data that helps us know if we are heading in the right direction. With Humbi by our side, we tapped not only the right data, but the expert analysis we were looking for."
This is the shape of competitive advantage in MSSP.
6. Fragmented Data Is Quietly Undermining Margins
Executives often talk about data quality as if it is an IT problem. It is not. It is a financial one. Poor integration forces teams to make decisions with partial visibility, and in MSSP, partial visibility tends to produce missed opportunities.
In a shared savings program that relies heavily on coordinated care, lagging or inconsistent data directly affects quality results and spending targets. Integration is now a performance requirement, not an upgrade.
7. Member Level Cost Data Is Becoming Negotiation Power
For years, payers had the upper hand in contract discussions because they had richer actuarial data. That dynamic is shifting.
Interoperability reforms mean providers can now analyze member-level cost patterns, compare them to regional benchmarks, and model savings scenarios with precision.
Organizations arriving at the table with data that quantifies risk, opportunity, and required adjustments negotiate better terms. Gains of 5 to 15% in shared savings splits are becoming common among early movers. Those without cost visibility will find themselves negotiating from a weaker position.
8. Patient Engagement Has Started Affecting Margins In A Direct Way
Engagement used to sound like a quality story. In MSSP, it is turning into a financial one. Patients who miss screenings, skip preventive care, or abandon medications cost more and generate lower shared savings.
Organizations treating engagement as part of financial strategy are seeing a clearer link between outreach, adherence, and year end results. Multi-channel outreach supported by timely data is becoming essential for meeting quality and savings goals.
9. Regulatory Velocity Requires Faster Modeling
CMS used to give organizations time to adjust. That rhythm is fading. Policy changes are arriving more quickly, and CMS-proposed downside risk tracks are forcing ACOs to model financial exposure earlier than they used to.
CFOs who wait for full clarity will find themselves reacting after the fact. The organizations winning the next cycle are the ones building repeatable ways to interpret, model, and act within days of new guidance rather than months.
10. Execution, Not Enrollment, Determines Performance
Joining a shared savings program is the beginning of the work, not the achievement. The real differentiator is how consistently an ACO executes on coordinated care, evidence based medicine, cost reduction, and data driven planning.
The gap between organizations that participate and organizations that perform is widening. In 2026, execution is becoming the metric that predicts who thrives and who survives.
Where Humbi AI Fits Into The 2026 Playbook
By 2026, actuarial intelligence is no longer optional for organizations in the Medicare Shared Savings Program. MSSP participation exposes ACOs to financial risk, shifting spending targets, shared losses, and performance rules that cannot be managed through manual models or retrospective analysis. The decisions CFOs make now will influence shared savings, downside exposure, and contract performance for years.
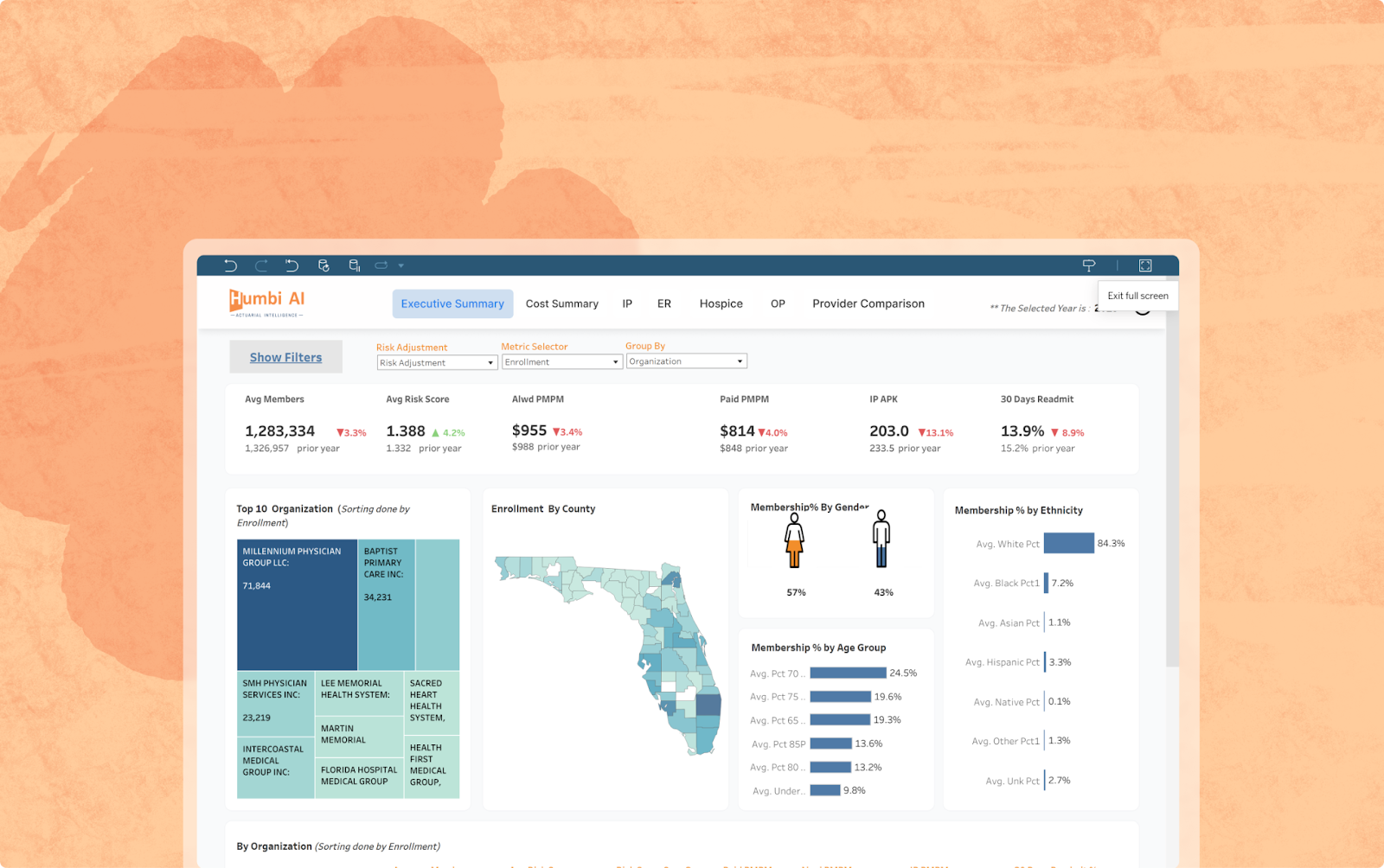
Humbi AI fills a capability gap that most organizations cannot build internally. It embeds actuarial models inside Innovaccer’s Healthcare Intelligence Cloud, giving finance, population health, and strategy teams a unified way to understand where value is created and where it is lost. With Humbi AI, CFOs can:
- Baseline true position against regional and national ACO peers
- Forecast shared savings, PMPM, and MLR outcomes across multiple scenarios
- Identify financially high-variance segments such as cost-rising cohorts, utilization outliers, and high-cost claimants
- Pinpoint spending patterns that deviate from expected actuarial behavior
- Strengthen payer contract negotiations with modeled evidence and competitive benchmarks
The impact is clarity. Leaders gain a decision layer that ties actuarial rigor to day-to-day operational and financial choices. Instead of reacting to CMS results at the end of the year, teams can see the drivers of savings and losses as they emerge.
Most MSSP renewals accelerate in mid and late 2026. The organizations that enter those conversations prepared, will be the ones that understand their risk-bearing profile, their performance variance, and their true market position. The organizations that wait will be negotiating from a position of uncertainty.
Humbi AI brings actuarial intelligence directly into your existing data environment so your teams can model risk, optimize contracts, and capture more value in MSSP and other value-based care programs. Book a demo to see how this works in practice.

